
A number of people have asked me for my opinion on COVID vaccination, despite the fact that I’m a theoretical chemist. Normally, I would point them to an immunologist or a doctor for advice, but therein lies the problem: one of the most common reasons for vaccine-hesitancy is a growing mistrust of “experts,” not just in medicine but in every field. Given the gravity of the situation, I’d like to make a case for COVID vaccination that requires minimal confidence in the government, public health officials, doctors, and scientists. Even if you believe that such lack of confidence is unwarranted, it may be useful to see how such a case can be made.
My argument will be based on three points.
- Death from COVID is roughly as likely as death from cancer. Consequently, to the same extent we seek to minimize the risk of death from cancer (even in young people, who don’t often die of cancer), we ought to seek to minimize the risk of death from COVID.
- Second, vaccines do indeed decrease the risk of COVID infection, hospitalization, and death. We can see this risk reduction clearly in recent data showing that the large majority of people currently being hospitalized for and dying of COVID are unvaccinated.
- The short-term risk of COVID vaccines (like the risk of all vaccines) is non-zero but small. Additionally, any wariness over the unknown long-term risks of the COVID vaccines has to be set against the long-term risks of COVID infection, which are equally unknown.
Note that I’m not making any argument whatsoever about masking, lockdowns, vaccine mandates or any other public policy. If these three points are true, then –in general– adults should voluntarily get vaccinated because the available evidence indicates that the benefits of vaccination outweigh the potential risks. But are these points true?
Assessing the Risk of Death from COVID
Imagine that we’re maximally skeptical about the risk of COVID. We’ve heard claims that millions of people worldwide have died of COVID, but how can we be sure that these claims are accurate? Perhaps people merely died “with COVID” but not “of COVID.” In other words, how do we know their deaths weren’t caused by heart disease or cancer and misattributed to COVID? Why think COVID tests are reliable? Can we be sure that what is being diagnosed as COVID isn’t just the seasonal flu?
To answer these questions, I’d like to focus on a very concrete number: excess deaths. Shown below is the raw data for the number of deaths in the U.S. over the last 5 years. We immediately notice that 500,000 more people died in 2020 than we’d expect based on the previous years’ totals. The natural question to ask is: what caused all these “excess deaths”?
| Year | Deaths |
| 2016 | 2,744,248 |
| 2017 | 2,813,503 |
| 2018 | 2,839,205 |
| 2019 | 2,854,838 |
| 2020 | 3,358,814 |
Figure 1 (below) sheds light on this question. The red line in Figure 1 plots these excess deaths by week by comparing weekly deaths in 2020/2021 to the average weekly deaths over the previous 5 years. Notice that excess deaths were not spread out evenly over the last 18 months. Instead, there are sudden spikes in March 2020, July 2020, and January 2021. This fact seems to rule out the idea that the excess deaths were caused by “deaths of despair” due to suicide or overdoses, which we’d expect to slowly increase as lockdowns or high unemployment persisted. Similarly, hospital closures might have delayed treatments for cancer or heart conditions, leading to deaths from these other causes. But these delays would not explain why tens of thousands of Americans died suddenly over a few weeks in March (and again in July and again the following January). These data also rule out the idea that excess deaths were caused by the seasonal flu. Contrary to what is sometimes claimed, doctors did continue to test for the flu in Spring 2020 and found that it virtually disappeared by April, just as we’d expect from previous flu seasons. In contrast, COVID tests show that COVID cases spiked in March 2020, July 2020, and January 2021, precisely when we see spikes in excess deaths. We see the same pattern globally when we look at excess deaths in countries like the U.K., Sweden, and Spain, and Israel.
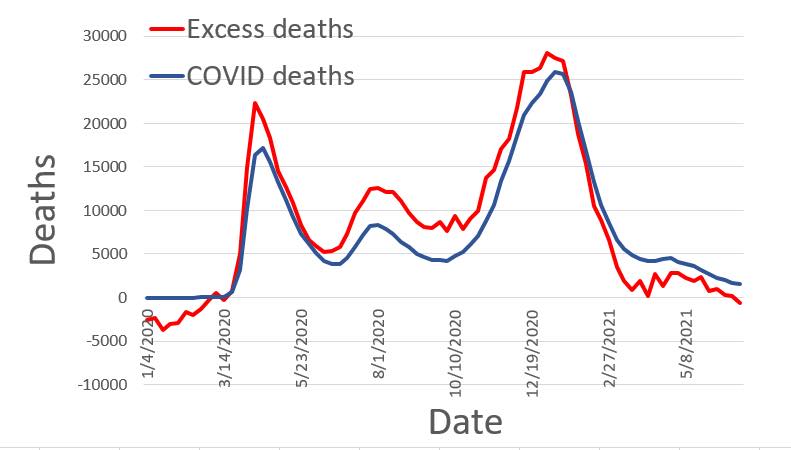
Even more significantly, the blue line in Figure 1 shows “COVID deaths” as recorded by the CDC during the same time period. The two plots are remarkably similar. Indeed, if anything, based on this graph, the CDC appears to undercount COVID deaths. Again, this is precisely what we’d expect if what the CDC labelled as “COVID deaths” did actually correspond to deaths caused by COVID. Anyone skeptical of this conclusion has to provide a plausible alternative explanation for why more than half a million Americans died over the last 18 months in waves that corresponded exactly to surges in COVID cases.
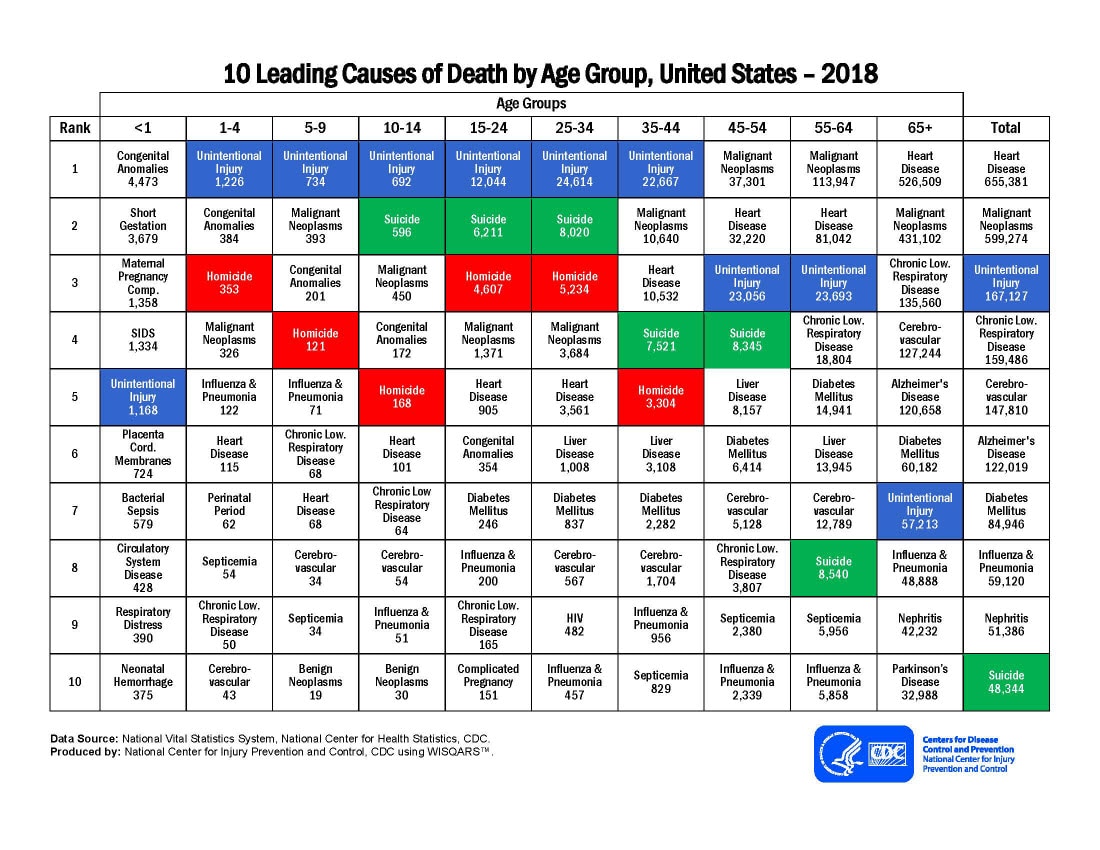
Substantiating the general reliability of these data allows us to estimate the risk of dying of COVID. As many people have pointed out (and as the CDC data shows), this risk is highly age-dependent. For example, a 75-85 year old is 230x more likely to die of COVID than a 18-29 year old. Consequently, when a 35-year-old hears that the fatality rate of COVID for his age group is only ~0.1%, he may assume that precautions are unnecessary. However, it’s helpful here to make a comparison to other causes of death to make the risk more concrete.
Although COVID deaths have spiked and receded periodically, it is roughly true to say that the likelihood of dying of COVID is roughly (within a factor of two) the same as the likelihood of dying of cancer. This comparison holds true for all age groups. How does that help us with risk assessment? It means that you should treat concerns about COVID with the same gravity you’d treat concerns about cancer. If there were a low-risk vaccine against cancer, virtually no one would reject it on the grounds that their age and overall health makes death from cancer highly unlikely. In the same way, we should not reject COVID vaccines merely on the grounds that COVID is unlikely to kill us. Instead, we should ask: are they effective? and are they safe? We’ll turn to those questions next.
Assessing the Effectiveness of Vaccines
Like any experimental drug or medical procedure, COVID vaccines were tested for efficacy. Of course, no vaccine is 100% effective and studies have consistently shown that “break-through infections” and death can still occur even in fully vaccinated people. But numerous studies have shown that COVID vaccines reduced both the likelihood of infection with COVID and the severity of the symptoms if a person was infected. For example, a clinical trial showed that vaccines were between 84% and 96% effective in preventing hospitalization in adults aged 65-74. However, I’m going to once again assume maximal skepticism towards such studies and instead focus on public data.
Here, emerging data on cases, hospitalization, and death are very important. A number of local governments have been tracking the number of COVID patients being admitted as a function of their vaccination status. In the U.S., as of August 2021, approximately 50% of all people were fully vaccinated. Consequently, if COVID vaccines had no effect whatsoever on the incidence or the severity of the disease, we’d expect that 50% of COVID hospitalizations would come from vaccinated people and 50% would come from unvaccinated people. What we see in reality, though, is starkly different.
For example, San Diego county has been releasing periodic COVID reports for months. As of Aug. 18th, 72.8% of San Diego Country residents were fully vaccinated. Thus, if vaccines were completely ineffective, we’d expect that around 70% of COVID cases, hospitalizations, and deaths would come from fully vaccinated individuals. However, between the dates of July 12th and Aug. 10th, only 8% of cases, 2% of hospitalizations, and 16% of deaths came from fully vaccinated individuals (see Figure 2 below).

In Louisiana, 38% of the population is fully vaccinated. Between July 29 and Aug. 4th, only 10% of the cases, 9% of the hospitalizations, and 17% of the deaths came from fully vaccinated individuals.
In Virginia, 53% of the population is fully vaccinated. Between July 27 and Aug. 2nd, only 5% of cases and 3% of deaths came from fully vaccinated individuals.
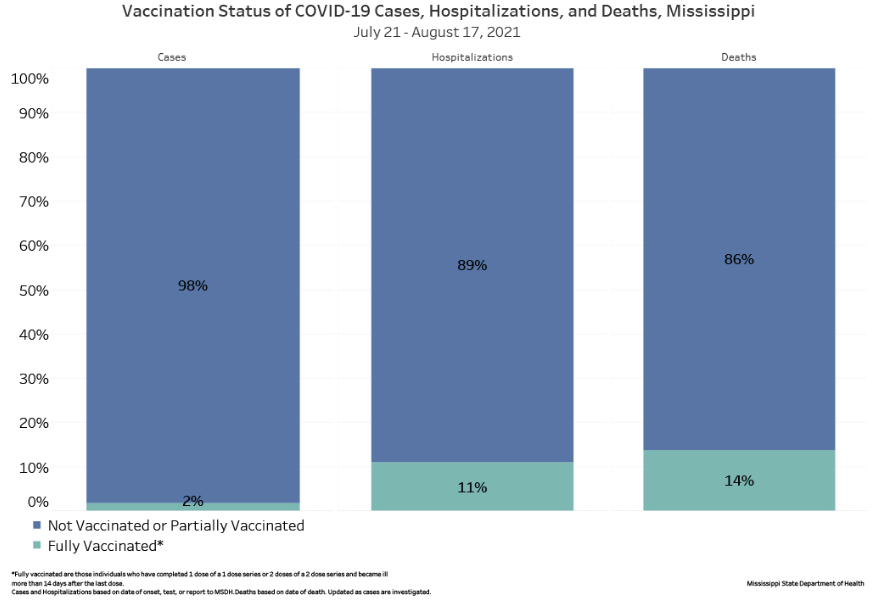
In Mississippi, 36% of the population is fully vaccinated against COVID. Between July 24th and Aug. 17th, only 2% of cases, 11% of hospitalizations, and 14% of deaths came from fully vaccinated individuals (see Figure 3 below).
In all these examples, and many others, fully vaccinated individuals are vastly underrepresented in terms of new cases, hospitalizations, and deaths, demonstrating the vaccines’ effectiveness. In fact, my analysis is conservative, since the elderly are significantly more likely to be vaccinated than the young and much more likely to die of COVID, which means that this analysis is likely skewed against the efficacy of the vaccine. Even so, it’s clear from these data that the vaccines offer real-world protection against both the virus and the severity of the disease if a person is infected. We don’t have to rely on scientific studies; we can see the importance of vaccination in rapidly-filling hospitals across the country.
Assessing the Risk of the Vaccine
Most people who are “vaccine hesitant” are not opposed to vaccination in general, but are wary of the COVID vaccine because it was developed far faster than most vaccines. As with all vaccines, there can be short-term side effects. Yet serious side-effects are extremely rare; for example, a study of over 2,000,000 vaccinated individuals reported only twenty cases of vaccine-related myocarditis (inflammation of the heart muscle), meaning that the risk of vaccination causing myocarditis was approximately 0.001% or 1 in 100,000.
An added complication in the case of COVID vaccines is that long-term side-effects have not been studied because the vaccines were only developed within the last year or so. Since these two concerns are distinct, I’ll treat them separately.
Since I’m again assuming a posture of skepticism towards scientific and medical claims, I won’t appeal to the many researchers who have concluded that the benefits of vaccination vastly outweigh the short-term risks. Instead, I’d like to take a practical approach. Since 50% of the U.S. population is fully vaccinated, the vast majority of people will personally know dozens of individuals who have been fully vaccinated. Similarly, since 10% of the U.S. population has contracted COVID, the vast majority of people will know at least several people who have contracted COVID. Hospitalization (~0.5% of the U.S. population) and death (~0.2% of the U.S. population) are rarer. However, the majority of people will still know someone who knows someone who has been hospitalized or has died of COVID.
Given these probabilities and how they will manifest in our social circles, we can then make a rough assessment of short-term risk by comparing two numbers: First, how many people do we personally know who know someone who has been hospitalized or has died as a result of COVID? Second, how many people do we personally know who know someone who has been hospitalized or has died as a result of the COVID vaccine? My experience here is probably typical. I personally know several people whose friends have died or have been hospitalized from COVID, but I don’t personally know anyone whose friends have been hospitalized or have died from the COVID vaccine.
Note that we should only include people we know personally, whom we have met face-to-face, for two reasons. First, personal friends and acquaintances are a more reliable sources of information than relative strangers from the Internet. Second, the Internet creates a tremendous amount of selection bias, since only sensational stories (but not common-place ones) are broadcast to millions of people.
Granted, this kind of experiential approach to risk is, well, risky. It’s always safer to use carefully collected data rather than our own experience. Yet carefully collected data indicates that serious vaccine side effects are so much rarer than COVID hospitalization that the vast majority of people will have the same kind of experiences I do. After all, around 1% of Americans who contract COVID will die of it. If COVID vaccines were as lethal as COVID, then mass vaccination would have already killed 1.6 million Americans. There is no evidence whatsoever that vaccines carry this kind of short-term risk.
The question of long-term risk is complicated by the fact that multi-year empirical studies of a year-old vaccine necessarily cannot exist. However, I’ll again take a practical approach. If we worry about the unknown long-term risks of the vaccines, then we should also worry about the long-term risks of COVID itself. After all, there are no multi-year empirical studies on the long-term risk of contracting COVID. For all we know, COVID itself carries a long-term, post-infection risk of infertility, heart disease, dementia, hypertension, stroke, and a host of other maladies.
It’s also worth observing that when past vaccines have been shown to have had rare, “long-term” side effects, these effects appeared within 2 months of the vaccination. So, in this sense, we do have “long-term” studies of the COVID vaccines, since they have been in widespread use for at least 6 months. Furthermore, several studies have suggested that COVID infection may carry long-term effects such as lower cognitive performance and increased resting heart-rate. For our purposes, we can simply observe that any fears about speculative long-term dangers from COVID vaccines are balanced out by speculative long-term dangers from COVID itself. If it’s reasonable to argue “I’m hesitant to be vaccinated because the COVID vaccine may have unknown long-term risks” then it’s also reasonable to argue “I’m hesitant to avoid vaccination because COVID infection may have unknown long-term risks.”
One final consideration should be added: my argument thus far has focused solely on a personal risk-benefit analysis, but broader considerations are also legitimate. For example, most estimates of R0 for COVID are between 2-3 which means that each infected person will infect 2-3 other people on average. Consequently, we ought to take into account not just whether we’re at risk but whether our actions put others at risk.
Imagine that Ford discovers a defect that causes their cars’ brakes to fail. They offer to replace the brakes in all their vehicles for free, but there is a small chance that the repair will cause other problems. If you drive a brand-new SUV with multiple safety features, you’ll be at significantly less risk than a person driving an ancient 1979 Ford Pinto with no seat-belts. So on the basis of a personal risk-benefit analysis, you might conclude that you can forgo the repair. But you should consider the fact that car crashes often involve multiple vehicles. If your brakes fail, you might well walk away safe; but you might kill other drivers or pedestrians.
Vaccination presents a roughly analogous situation. Even if we are personally willing to take our chances as a member of a relatively low-risk group, we should also consider the possibility that we’ll pass a life-threatening illness on to someone else in a higher-risk group.
Summing Up
Although I’m fully vaccinated, I’m sympathetic to many of the concerns of the vaccine-hesitant. I understand people’s skepticism towards institutions. When 1000+ health professionals insist that stay-at-home orders should not be applied to people “protesting against systemic racism” and when CNN affirms in a news article that there is “no consensus criteria for assigning sex at birth,” many people rightly worry that medicine and public health policy have become politicized
While it’s fair to express such skepticism, we need to be even-handed. If we refuse to blindly accept the dictates of -say- John’s Hopkins or the WHO, we should not blindly accept the proclamations of that guy on YouTube or that headline we saw on Twitter. One-sided skepticism is not skepticism; it’s just selective credulity. Instead, we have to always ask what the data say and draw conclusions consistent with them.
I also understand people’s frustration over draconian restrictions on public gatherings (conveniently ignored by many of the politicians imposing them) and ever-changing CDC guidelines. But in this article, I am in no way making an argument about public policy. You can staunchly oppose -say- vaccine passports and still passionately commend voluntary vaccination. Indeed, as Americans, we normally pride ourselves on this distinction: I can urge others to vote for a particular candidate, go to church, or adopt certain beliefs while abhorring any law that would compel these actions.
In the end, I suspect the biggest obstacle to vaccination for many people is trust. We’re swimming in a sea of misinformation on both sides and many of us don’t know where to turn. For that reason, if you’re unpersuaded by the arguments listed above, I urge you to seek out someone with professional expertise in this area whom you also know personally. They may be able to address the questions I’ve left unanswered and their assessment should certainly carry more weight with you than the musings of a random theoretical chemist with a blog.
Alternatively, if you’re an advocate for vaccines, I recommend that you take people and their concerns seriously. Sneering at people is no way to persuade them. Shaming them and attempting to coerce them may only make them dig in their heels. The idea that the ranks of the vaccine-hesitant are solely populated by uneducated, white religious conservatives is simply false. People are complex. Take time to listen to them, to find areas of agreement, and to make your case with gentleness and respect. Beware of winning the argument and losing the person.
Related articles:

{kind=link}